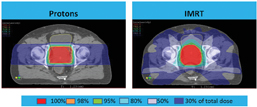
Protons vs. IMRT
We are witnessing a new era in proton therapy research, with an unprecedented number of clinical studies under way. For three decades, research has focused heavily on pediatric tumors and tumors of the brain, spine and prostate, establishing that proton therapy is efficacious, enables precise targeting of tumors permitting higher doses of radiation with few short- and long-term side effects, and maintains a high quality of life for patients.[1-9] The treatment also has been shown to reduce the likelihood of treatment-related malignancies.[10] Researchers now are exploring the clinically meaningful benefit of proton therapy in diseases of high incidence, particularly lung and breast cancer, where the precision and limited side effects can provide effective treatment with significant long-term benefit to the patient. Initial results prove hopeful, especially for lung cancer, which remains the No. 1 cancer killer of both men and women.[11]
Pediatric and Prostate: Focus on Quality of Life
The research on proton therapy’s efficacy and reduction in side effects has been complemented in recent years by quality of life studies. A paper by Merchant et al notes that in comparison to photon radiation, proton therapy lessens the distribution of low and intermediate doses to areas of the cerebrum in children receiving treatment for brain tumors.[12] Modeling suggests this reduction in radiation to sensitive and critical areas of the developing brain will result in fewer negative cognitive affects in children. Longitudinal models show children who receive proton therapy for medulloblastoma and craniopharyngioma will have significantly higher IQ scores than those treated with photons. This is significant as the more effective we are in treating pediatric malignancies, the more we must be mindful of the aftereffects of treatment and the future of the survivors of childhood cancer.
Research on prostate cancer treatments involving protons and other modalities increasingly is focusing on immediate and long-term quality of life, which is of prime concern to men as they make treatment choices. Several newer studies have shown proton therapy offers significant benefits. A study by Hoppe et al surveyed 262 young (age 60 or under) prostate cancer patients prior to proton therapy and every six months after, using the Expanded Prostate Index Composite (EPIC) and International Index of Erectile Function (IIEF) questionnaires.[13] At two years post-treatment, this group of young men had excellent outcomes in regards to erectile dysfunction and urinary incontinence. While potency rates declined by 11 percent from baseline, 94 percent of a subset of relatively healthy men (baseline IIEF of >21, body mass index of <30 and no diabetes) remained potent. Only 1.8 percent of men required a pad for urge incontinence. A multi-institutional study compared EPIC responses of 1,090 men with prostate cancer to a control group of 112 nontreated men and determined both groups had similar quality of life scores regarding urinary function/bother and bowel function/bother.[14] Sexual function/bother scores were slightly lower for treated men.
Two highly publicized research papers seem to contradict the consistently positive results being reported in multiple well-regarded studies. However, it is important to note that these were not controlled clinical studies and that researchers analyzed Medicare data instead of actual patient reports or responses.[15,16]
Many more prostate trials are under way or continuing, including a randomized controlled trial comparing side effects of proton therapy vs. intensity-modulated radiation therapy (IMRT). Massachusetts General Hospital and the University of Pennsylvania currently are recruiting low- and low-intermediate risk prostate cancer patients for the trial.
Future Direction: Lung
Via its ability to target the tumor with more specificity, to reduce radiation to surrounding healthy tissues and therefore to enable higher-dosage treatment, proton therapy is poised to play an important role in the treatment of non-small cell lung cancer (NSCLC). Until we are able to identify lung cancer earlier in its course, combination radiation and chemotherapy likely will remain part of the treatment regimen for many NSCLC patients. Combining proton therapy and standard chemotherapy has been shown to be efficacious, reporting promising survival rates and lower rates of pneumonitis and esophogitis.[17,18]
Comparing toxicity of proton therapy/chemotherapy in 62 Stage III NSCLC patients to similar-size groups of patients treated with 3D-CRT/chemotherapy and IMRT/chemotherapy, Sejpal et al found proton patients suffered significantly lower rates of severe pneumonitis (2 percent with protons vs. 30 percent and 9 percent for photon modalities) and esophagitis (5 percent vs. 18 percent and 44 percent) despite receiving higher radiation doses (74 Gy (RBE) protons vs. 63 Gy for two photon modalities).[17] Chang et al followed 44 Stage III NSCLC patients treated with 74 Gy proton therapy and concurrent standard chemotherapy and reported a median survival of 29.4 months.[18] They also found that esophagitis, pneumonitis and late toxicity were improved in these patients compared to results of other radiation therapy studies. MD Anderson and Massachusetts General Hospital have now launched a National Cancer Institute-funded randomized controlled trial comparing proton/chemotherapy to IMRT/chemotherapy in this group of patients.
Future Direction: Breast
Breast cancer presents many challenges for radiation oncologists. Radiotherapy is efficacious in patients with breast cancer, but because it can expose heart, coronary vessels and lungs to excess radiation, it can be associated with lung fibrosis, secondary malignancies and, in women with left-side breast cancer, increased risk of coronary artery disease and cardiac mortality. Proton therapy addresses some of these treatment-related side effects. A prospective study by MacDonald et al analyzed nine patients with locally advanced breast cancer who had a mastectomy and received proton therapy post chemotherapy. The chest wall and regional lymph nodes were treated with excellent sparing of the cardiopulmonary structures.19 Average mean dose to the heart, left ventricle and lung was 0.44, 0.09 and 6 Gy respectively, and average V20 to the heart, lung and left ventricle was 0 percent, 0 percent and 13 percent.
In a dosimetric comparison study using four different plans — proton therapy, 3D-CRT, IMRT and helical tomotherapy (tomo) — Moon et al found that proton therapy provided significantly less radiation to normal tissues compared to the other therapies.20 The average ipsilateral lung volume receiving 20 percent of the prescribed dose was significantly lower in proton therapy (0.4 percent) vs. IMRT (2.3 percent), 3D-CRT (6 percent) and tomo (14.2 percent). The average heart volume percentage receiving 20 percent of the prescribed dose in left-sided breast cancer was 0 percent in proton therapy, compared to 1.5 percent (3D-CRT), 1.2 percent (IMRT) and 8 percent (tomo). Similarly, Ares et al prepared treatment plans for 20 left-sided breast cancer patients and determined that proton therapy offered improved target coverage while comparatively reducing doses to organs at risk vs. IMRT and 3D-CRT.21 In subsequent increasingly complex locoregional volumes, low (V5) left lung and cardiac doses were reduced by a factor of >2.5, and cardiac doses (V22.5) were reduced by a factor of >20 lower with proton therapy compared with IMRT. The studies found the benefit of proton therapy was greater as target complexity increased.
Proton Therapy: Ever-Evolving
The growth of proton therapy research in combination with a number of innovations indicates an expanding role for proton therapy. This is due in part to new technologies that enable even better precision. One of the most exciting advances is pencil beam scanning (PBS), which further increases dose conformality, depositing even more radiation directly in the tumor, while sparing surrounding healthy tissue. The advantages of PBS are numerous and will enable more patients to benefit from proton therapy. It decreases or nearly eliminates neutron scatter dose, especially important in pediatric cancer treatment. PBS increases the ability to dose paint, further sparing normal organs in close proximity to high-dose tumor volumes. It is also faster — even very complex patients require only 30-minute time slots — meaning we can schedule and treat more patients.
Paralleling PBS are other advancements, such as technologies enabling the downsizing of the hardware. Improvements in imaging are allowing better treatment planning, permitting adaptive therapy by allowing optimization of treatment as the tumor shrinks over time. These various advancements allow us to reduce the cost of proton therapy — due to shorter planning and treatment time as well as smaller equipment and facilities — benefitting patients, payers, the healthcare system and society overall.
Researchers undoubtedly will document how these advances affect outcomes and add their findings to the ever-expanding number of studies on the use of proton therapy. We will continually assess this growing body of knowledge to determine how proton therapy can be most effective and beneficial in the treatment of patients dealing with the devastating diagnosis of cancer.
Eugen B. Hug, M.D., is medical director and chief medical officer for ProCure Treatment Centers, and is a world-renowned expert in proton radiotherapy. A pioneer in the use of proton therapy for pediatric tumors, Hug has spent more than 20 years treating patients, teaching, writing and conducting research. He was principal or co-investigator of various clinical trials, including studies focusing on proton therapy. He is widely published in radiation oncology periodicals and books, authoring numerous journal articles or chapters. Additionally, he
is a sought-after lecturer and teacher at international medical meetings, symposia and seminars.
References:
1. Mendenhall N, Li Z, Hoppe B, et al. “Early outcomes from three prospective trials of image-guided proton therapy for prostate cancer.” Int J Radiat Oncol Biol Phys. 2012;82(1):213-21.
2. Zietman A, Bae K, Slater J, et al. “Randomized trial comparing conventional-dose with high-dose conformal radiation therapy in early-stage adenocarcinoma of the prostate: long-term results from proton radiation oncology group/American College of Radiology 95-09.” J Clin Oncol. 2010;28(7):1106-11.
3. Zietman A, DeSilvio M, Slater J, et al. “Comparison of conventional-dose vs high-dose conformal radiation therapy in clinically localized adenocarcinoma of the prostate.” JAMA. 2005;294(10):1233-9.
4. Komaki R, Sejpal S, Wei X, et al. “Reduction of bone marrow suppression for patients with Stage III NSCLC treated by proton and chemotherapy compared with IMRT and chemotherapy.” Particle Therapy Cooperative Group 47. 2008;O10:14.
5. Mayahara H, Murakami M, Kagawa K, et al. “Acute morbidity of proton therapy for prostate cancer: the Hyogo Ion Beam Medical Center experience.” Int J Radiat Oncol Biol Phys. 2007;69(2):434-43.
6. Steneker M, Lomax A, Schneider U. “Intensity modulated photon and proton therapy for the treatment of head and neck tumors.” Radiother Oncol. 2006;80(2):263-7.
7. Lee C, Bilton S, Famiglietti R, et al. “Treatment planning with protons for pediatric retinoblasta, medulloblastoma, and pelvic sarcoma: how do protons compare with other conformal techniques?” Int J Radiat Oncol Biol Phys. 2005;63(2):362-72.
8. Fowler J. “What can we expect from dose escalation using proton beams?” Clin Oncol. 2003;15(1):S10-15.
9. Miralbell R, Lomax A, Cella L, Scheider U. “Potential reduction of the incidence of radiation-induced second cancers by using proton beams in the treatment of pediatric tumors.” Int J Radiat Oncol Biol Phys. 2002;54(3):824-9.
10. Chung C, Keating N, Yock T, Tarbell N. “Comparative analysis of second malignancy risk in patients treated with proton therapy versus conventional photon therapy.” Int J Radiat Oncol Biol Phys. 2008;72(1 Suppl):S8.
11. American Cancer Society. Cancer Facts & Figures 2013. Atlanta: American Cancer Society; 2013. Accessed Feb. 11, 2013 at
www.cancer.org/acs/groups/content/@epidemiologysurveilance/documents/do…
12. Merchant T, Hua C, Shukla H, et al. “Proton versus photon radiotherapy for common pediatric brain tumors: comparison of models of dose characteristics and their relationship to cognitive function.” Pediatr Blood Cancer. 2008;51:110-7.
13. Hoppe B, Nichols R, Henderson R, et al. “Erectile function, incontinence, and other quality of life outcomes following proton therapy for prostate cancer in men 60 years old and younger.” Cancer. 2012;118(18):4619-26.
14. Lee A, Levy L, Rossi, C, et al. “Multi-institutional patient-reported quality of life after proton therapy for prostate cancer compared to nontreated men.” Int J Radiat Oncol Biol Phys. 2012;84(Suppl 3):S646-7.
15. Sheets N, Goldin G, Meyer A, et al. “Intensity-modulated radiation therapy, proton therapy, or conformal radiation therapy and morbidity and disease control in localized prostate cancer.” JAMA. 2012;307(15):1611-20.
16. Yu J, Soulos P, Herrin J, et al. “Proton versus intensity-modulated radiotherapy for prostate cancer: patterns of care and early toxicity.” J Natl Cancer Inst. 2013;105(1):25-32.
17. Sejpal S, Komaki R, Tsao A, et al. “Early findings on toxicity of proton beam therapy with concurrent chemotherapy for non-small cell lung cancer.” Cancer. 2011;117(13):3004-13.
18. Chang J, Komaki R, Lu C, et al. “Phase 2 study of high-dose proton therapy with concurrent chemotherapy for unresectable Stage III non-small cell lung cancer.” Cancer. 2011;117:4707-13.
19. MacDonald S, Specht M, Isakoff S, et al. “Prospective pilot study of proton radiation therapy for invasive carcinoma of the breast following mastectomy in patients with unfavorable anatomy – first reported clinical experience.” Int J Radiat Oncol. 2012;84 (Suppl 3):S113-4.
20. Moon S, Shin K, Kim T, et al. “Dosimetric comparison of four different external beam partial breast irradiation techniques: three-dimensional conformal radiotherapy, intensity-modulated radiotherapy, helical tomotherapy, and proton beam therapy.” Radiother Oncol. 2009;90:66-73.
21. Ares C, Khan S, Macartain A, et al. “Postoperative proton radiotherapy for localized and locoregional breast cancer: potential for clinically relevant improvements?” Int J Radiat Oncol Biol Phys. 2010;76(3):685-97.

 July 28, 2026
July 28, 2026 






")
