
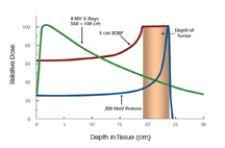
The maximum dose is known as the Bragg Peak. For protons, the dose immediately beyond the Bragg Peak is zero, sparing healthy tissue from damage.
Even when it is a matter of life and death – access to the best care available is still a matter of dollars and cents. That is the case with proton radiation therapy – a noninvasive, painless procedure that destroys tumors more effectively than conventional forms of radiation and reduces damage caused to the healthy tissue, yet few patients are treated with it.
There are only five clinical sites in the U.S. that offer proton radiation therapy, despite a growing demand for it. The biggest obstacle is the enormous investment required to implement the technology and build its infrastructure. On the high end, for example, the initial capital investment to build the M.D. Anderson Cancer Center - Proton Therapy was $120 million.
To date, only a few large research hospitals and facilities have had the financial backing for such a capital-intensive investment, shutting out not only smaller hospitals but also patient access to better care. However, recent advances in accelerator technology and a smaller footprint for both the equipment and the facility are expected to lower the overall price tag of proton therapy and open closed doors to patients nationwide.
Proton vs. Conventional Radiation Therapy
The real advantage of proton therapy lies in its precision. With conventional external beam radiation therapies, the photon beam delivers its peak radiation dose shortly after entering the body, and diminishes gradually as it travels through the tumor and exits the body. With proton therapy, the dose of radiation deposited by the proton beam increases gradually before suddenly rising to a peak and then dropping to zero; the maximum dose is known as the Bragg Peak. The proton beam can be modulated so that a series of Bragg Peaks create a dose pattern that fully conforms to the tumor volume.
For protons, the net dose to the healthy tissue surrounding a tumor is much less than that to the tumor itself, thus sparing the normal tissue in this area. The dose immediately beyond the Bragg Peak is zero, which allows normal tissues posterior to the tumor to be spared. As a result, both acute and long-term side effects that are common with photon therapy can be markedly reduced or eliminated.
“With the proton, the dose drops from 100 percent to zero over a distance of about a sixteenth of an inch or a
couple of millimeters, so you can come right up against a critical organ, kill the tumor and not damage that critical organ. You can do a better job of tailoring the radiation to the tumor and causing a lot less collateral damage to healthy tissue,” explained John Cameron, Ph.D., a particle therapy physics pioneer who was pivotal in the development of the Midwest Proton Radiotherapy Institute in Bloomington, IN, and founder of ProCure Treatment Centers Inc.
Currently, many radiation oncologists apply mixed therapy, dividing the treatment between photon radiation and a proton boost, allowing clinicians to use the proton resource for
more patients.
“The first reason for using both photon and protons for part of the treatment is an economics reason, namely that protons are a rare resource, and if you can use the protons to boost the dose to the tumor volume, you can treat more patients with a proton boost,” said Dr. Cameron. “If a patient is getting 80 Gray into a trigger, you give the first 50 with photons, then give a proton boost with 30, and you spend a lot less time at the proton machine.” A proton boost is also implemented when there is uncertainty of the location of the tumor or if the tumor has extended beyond the well-known area.
Experts anticipate that even if proton therapy becomes more available, initially, complementary use of photons and protons will continue. “The likely scenario is that proton therapy will supplement an existing radiotherapy program,” said Spencer Sias, Varian Medical Systems, vice president for corporate communications. “Where you get part of your treatment from standard photons and then you get a proton boost.”
Downsized Model Made Affordable
Worldwide, nearly 50,000 cancer sufferers have taken advantage of photon radiation therapy to treat common types of cancer, including head and neck, prostate, breast, lung, colorectal and brain tumors. Yet in the U.S., proton therapy is still known as the rich man’s cancer treatment. That is expected to change, however.
“Proton therapy was once thought to be only for the very wealthy, but now people are looking at taking cost out of it to make it so it is more affordable and available to more people and a broader number of centers,” said Sias. “The interest in proton therapy has heightened in the last year because centers like M.D. Anderson just put in a new center and others are now taking interest. And there are at least 30 centers that are either in operation or planned.”
Re-engineered systems have reduced the size of the accelerator, requiring less space, less treatment rooms and smaller infrastructures to house the systems. By downsizing the overall footprint, the cost of building and maintaining a proton therapy center drops significantly and should broaden access.
Tufts-New England Medical Center in Massachusetts announced last year that it will apply proton beams in treating cancerous tumors. The hospital plans to use a new unit called the Clinatron-250 being developed at MIT (Massachusetts Institute of Technology) that is more compact and more cost effective.
Unlike conventional proton systems that use a synchrotron or isochronous cyclotron as the particle accelerator, the new device will deliver protons from a synchrocyclotron – a cyclotron in which the frequency of the driving RF electric field is varied to compensate for the mass gain of the accelerated particles as their velocity begins to approach the speed of light. There is reportedly no clinical difference between the proton beam that the Clinatron-250 delivers from that of any other system. The preliminary price is a mere $20 million, a fraction of the usual price.
“It has been the dream of every radiation oncologist to have access to a proton beam, but this has been limited because of the enormous expense associated with these facilities,” said David E. Wazer, Ph.D., radiation oncologist in chief at Tufts-New England Medical Center.
The systems are expected to be available for clinical use by 2008 and Tufts aims to be the first hospital in Massachusetts to offer the new unit. The hospital projects it will treat 253 patients in 2009 and as many as 356 by 2012. Developers of the new systems anticipate that the facilities that already have the larger proton therapy devices installed would be inclined to purchase the new units to reduce patient backlog.
Although Clinatron-250 is pending FDA clearance, the manufacturer of the system, Still River Systems, a development-stage company based in Littleton, MA, already has a contract with Barnes-Jewish Hospital in St Louis, MO, to construct a one-room proton-therapy facility onsite. Recently, American Shared Hospital Services, a turnkey radiation oncology provider, and M.D. Anderson Cancer Center Orlando have also entered into an agreement to purchase a unit by either 2008 or 2009. The number of clinics that can consider putting in a system like this will expand, says Spencer. “Proton Therapy systems will apply to large centers, but they do not need to be an M.D. Anderson,” he noted.
Superconducting Cyclotron Accelerates Proton Trend
With new technology carving out room for proton beams in radiation therapy, Varian Medical Systems spent approximately $30 million to acquire 100 percent of ACCEL Instruments GmbH, a privately-held supplier of proton therapy systems for cancer treatment and scientific research instruments. The acquisition will enable Varian to offer products for delivering image-guided, intensity modulated proton therapy for selected cancer patients.
Proton therapy has traditionally been a multi-room system where you build a whole building and one of the rooms holds the cyclotron accelerator or cyncrotron, explains Sias. The proton beam is routed to a treatment room to the gantry, which delivers the dose to the patient.
“The problem is the size of the construction project drives the cost up to $150 million or more,” Sias indicated. “Why use multiple rooms and why not make it smaller to take cost out. Now a cyclotron with a single treatment room can be taken down to a $30 million range, making it more affordable to a broader range of centers.”
What appealed to Varian about ACCEL, notes Sias, was its superconducting magnet technology, a superconducting medical cyclotron used for steering the beam. This technology makes it possible to shrink the size of the system and bring cost down. Another attribute of ACCEL’s technology is its scanning beam technology, which enables intensity modulated proton therapy (IMPT), a more precise technique for delivering proton therapy compared to other technologies. IMPT allows you to reduce the neutron spread, reduce scatter and do a better job of dose distribution. Sias added, “We can also take the technology and scale it up, adding in Varian’s proton treatment planning to create a total proton therapy solution, which complements what we already do in photon and electron radiotherapy.”
Varian says it is responding to a need for proton therapy that has been expressed by its customers. “We do believe that [proton therapy] was probably a $250 million market last year, and that Varian can have a business that approaches that size over time,” indicated Sias.
Community Access to Proton RT
One man’s mission to increase the availability of proton therapy for cancer patients has manifested itself in a business model that targets private practice oncology centers. Dr. Cameron, who founded ProCure Treatment Centers Inc. in 2005, offers an approach that involves building partnerships with the nation’s leading radiation oncologists and community hospitals to create a network of proton therapy centers in communities across the U.S.
Today, the existing five proton therapy facilities in the U.S. treat just 5,000 to 6,000 patients a year, while there are about 800,000 patients who undergo radiation therapy – that means less than one percent of all patients receive proton therapy. According to Dr. Cameron, between 20 and 30 percent of all cancer patients would benefit significantly from having protons for all or part of their treatment. “So we really have a demand of around 25 percent and a one percent supply,” said Dr. Cameron.
Since 80 percent of cancer patients seek treatment at large universities and hospitals, Dr. Cameron believes that there is a need for local proton therapy centers. According to ProCure CEO Hadley Ford, that is why ProCure is focusing on forming partnerships at the community level. “Our dream is to make proton therapy accessible to everyone who would benefit from the treatment,” said Ford.
Private Practice Breaks New Ground
Cancer is the second leading cause of death in Oklahoma with approximately 7,500 Oklahomans dying each year from the disease. As there are no proton radiation therapy facilities in the state, Oklahoma families have been forced to travel to other parts of the country for this treatment.
Two leading radiation oncology practices in Oklahoma City, Radiation Medicine Associates (RMA) and Radiation Oncology Associates (ROA), are pioneering the first private practice proton therapy treatment center in Oklahoma and the nation with the help of ProCure.
“The physical quality of proton particle therapy is superior and limits the exposure of normal tissues to the effects of radiation,” indicated William C. Goad, M.D., who formed Radiation Medicine Associates in 2001 with John Taylor, M.D. “When proton therapy is combined with chemotherapy, patients will have fewer side effects and complications that may limit their ability to tolerate treatment for the best results. Clinical studies demonstrate that proton therapy reduc[es] side effects and improv[es] the outcome of treatment for cancer patients.”
The goal of the new, four-room 55,000 square-foot facility, scheduled for completion in 2009, is to give an additional 1,500 cancer patients per year access to proton therapy.
The oncologists deliver the expert care, while ProCure provides management support, complete design, construction, operation and maintenance of proton therapy treatment centers. “The most important thing that we bring to table is the financial package and a plan to the radiation oncology group or community hospital that is economically viable. We make it technologically viable with the construction of the facility,” said Dr. Cameron. “From the radiation oncologists’ perspective, their life is not changed significantly; they are still determining radiation volumes and the tumors they want to radiate, which is the same for conventional therapy. We make life for them very similar.”
The new proton therapy center will install equipment, valued at around $50 million, supplied by IBA (Ion Beam Applications), a leader in particle therapy. “Proton therapy is increasingly accepted as the next big advance in cancer treatment using radiation,” said Pierre Mottet, IBA’s CEO. “ProCure has developed a unique concept to make this new technology available to community hospitals and private practices based on a smart financing package and integrated approach. We expect that their concept will be key in providing access to proton therapy for many hospitals, physicians and patients in the U.S.”
With more compact technology, revised facility layouts and a private practice business model, proton therapy may soon reach the rest of the patient population.

 July 16, 2026
July 16, 2026 






