
When Radiology Associates has a problem that needs to be solved it creates a multidisciplinary team drawn from every aspect of its operation involved in the problem. Together, the team analyzes the problem and suggests experimental ways of addressing it that could work for all involved.
If you are a partner in, or manager of, a private radiology practice, this is probably your reality today: You have a large overhead to maintain, from buildings and staff to expensive equipment that needs replacing as the technology evolves. Meanwhile, you are facing one reimbursement cut after another. Since 2006, Medicare alone has slashed radiology reimbursements a dozen times, with more cuts scheduled due to healthcare reform. Many private payers have also followed Medicare’s lead.
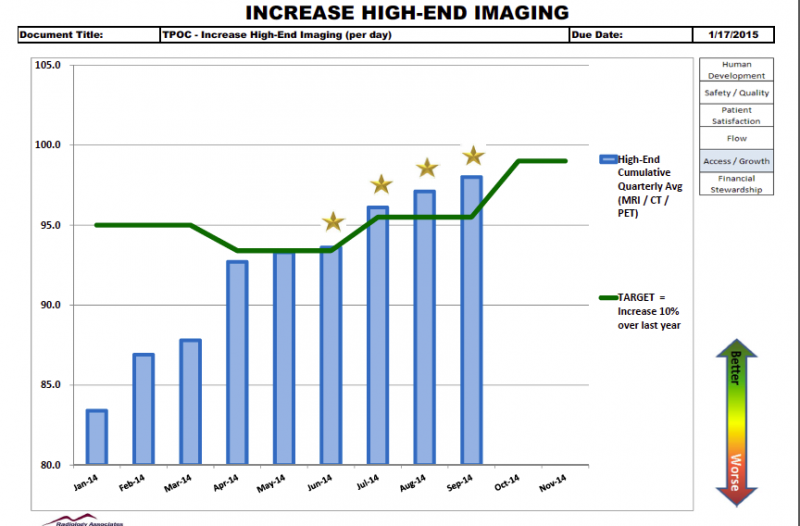
Expenses up, revenues down — what can you do? The approach that has worked for our practice is to expand our capacity, by combining lean transformation concepts with the sophisticated tools and metrics provided by advanced health information technology.
Our business, Radiology Associates (RA), is based in San Luis Obispo and covers the central coast of California. We are now growing about 10 percent per year. As just one factor in that success, some RA radiologists have increased their reading productivity by 50 percent. Our formula can be applied by many radiology practices.
The framework for our growth comes from lean transformation. Lean does not seek growth at the expense of quality. In fact, it does the opposite — using continual analysis of an organization’s management systems and workflows to free up bottlenecks and eliminate wasted steps. The resulting efficiency and productivity gains then improve the quality and reliability of the services the organization delivers to customers. While lean is accomplishing that, it also lowers costs.
The second component of our formula is to use state-of-the-art radiology information systems designed by people who understand health information technology workflows and business needs. Our IT generates metrics that are vital to our lean project. It enhances our radiologists’ and technologists’ productivity because the technology (from DR Systems) is efficient to use, from reading to report generation.
In addition, we employ tools built into our information systems that make us more efficient and productive and therefore advance our lean goals. That said, those tools are only helpful when you use them. So we’ve also invested the time to become power users.
Here are some examples of how the combination of lean transformation and health IT work together to help us grow:
Radiologist worklists: RA operates three centers, staffed by a total of seven radiologists. But before we had our current IT, we had no good way to create an electronic, RA-wide worklist. Instead, each center maintained its own worklist, with radiologists there responsible for that list alone. If one center was overly busy and another had downtime, we could not electronically distribute the load between centers. Nor had we found an efficient way to divide the load by sub-specialty.
Our current IT solves both of these issues at once. We read from a unified worklist, with the next available radiologist at any center usually getting the next unread case. The technology has various filters that can make the process more efficient still. If the case is more appropriate for a sub-specialist, it can be assigned to that doctor and the available radiologist will get the following case in the queue.
Alternatively, if, say, we prefer that a neuro sub-specialist read only neuro cases, we can set a filter accordingly. All of these automatic means of divvying up workloads create time savings that add up to increased capacity. Again, per lean, we want to maximize productivity even as we increase quality. Our unified worklist features make that possible.
Report process customization: Before an exam is read, a radiologist needs certain facts gathered about the patient’s clinical history that will inform the interpretation of the image. We also want to know where the prior exams are located. We utilize a tool in our RIS/PACS that reminds technologists of the questions to ask in each patient interview, using exam-specific instructions. After they gather the requested information in their interviews, another tool in the RIS/PACS is used to automatically map the information into the report.
This approach not only increases technologist and radiologist efficiency, but also increases patient satisfaction. That is because patients see on their report that the information they gave the technologist was considered by the radiologist, and not just lost on some misplaced paper form.
We have numerous other ways to customize our report generation. For instance, whenever we find ourselves repeatedly adding certain information to a report — say, because professional guidelines changed — we can create a custom electronic button to capture that process. The buttons are organized on a toolbar that reminds every radiologist to include in the report the information represented by the button. Clicking on the button populates the report with the information indicated by the button, complete with a reference to the associated guideline. This feature reduces variation in our reports, which our referring physicians appreciate because it helps them navigate through the documents more easily.
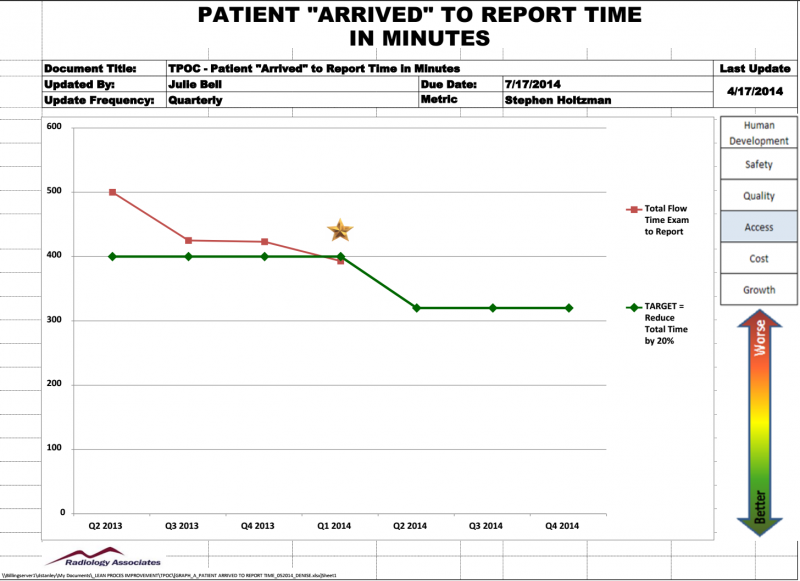
Report turnaround time (TAT): Our goal is to minimize the span between the time patient arrival is entered into the RIS, and the time the report arrives in the referring physician’s EHR. We document those starting and arrival times with metrics from our IT.
To cut that time span, we break it down into all the workflows that comprise it, one modality at a time. Take our X-ray workflow, for instance. First, we flow-charted the process, which made us aware of a bottleneck involving the time it took patients to complete paperwork. Elderly or ill patients can struggle with paperwork, holding up the entire operation. We eliminated that bottleneck by having staff interview the patients for basic information and then enter the info into the IT system.
When you multiply by the number of patients over the course of a day or week, this little time-saver adds up to a truly significant total. And by saving ourselves time, we’re also saving our patients time, which improves their experience with us.
Multidisciplinary problem-solving: The previous examples show how we are utilizing lean and our IT together to grow our capacity. Here is an example of using lean alone:
In many organizations, changes in process are dictated from on high, by business owners and managers. Those changes may make sense to those who ordered them, but they often have unintended, negative consequences for frontline workers. Those consequences can then undermine the goal of improving efficiency and productivity.
Lean is based on the idea that frontline workers know the work the best. Therefore, no substantial change should be considered that doesnot include their insights. So when we have a problem we want solved at RA, we create a multidisciplinary team drawn from every aspect of our operation involved in the problem — patient registration, scheduling, imaging, whatever. Team members are relieved of their regular duties and sequestered in a classroom with a consultant who moderates. Everyone checks their titles at the door. Together, the team analyzes the problem and suggests experimental ways of addressing it that could work for all involved.
We hold such meetings on a monthly basis, targeting a different problem each time. Besides being effective for achieving constant improvement, this approach boosts morale for frontline staff, who feel that they have been heard and are thus highly motivated to make a proposed solution work. Our inspired team is figuring out how to work smarter, not harder.
All of the above examples show the comprehensive process by which we examine every segment of every major workflow for potential savings. But once more: savings and quality are twin goals. Sacrificing quality for efficiency or productivity would undermine our goals. Instead, using advanced IT and lean philosophy, we are able to grow the bottom line and also do a better job of meeting the needs of patients and the physicians who refer to us.
Editor’s note: Stephen R. Holtzman, M.D., M.S. is CEO of Radiology Associates (RA) in San Luis Obispo, Calif. He is secretary for the California Radiological Society and a member of the Quality Improvement Team for the Society of Interventional Radiology (SIR). In addition to his medical degree from Dartmouth Medical School, he holds an M.S. degree from Dartmouth in evaluative clinical sciences. Holtzman is a member of the American College of Radiology (ACR), Radiological Society of North America (RSNA), California Radiological Society, American Medical Association (AMA), and the SIR and a former member of the American Board of Radiology's Expert Panel in Cardiovascular Imaging.
 April 25, 2024
April 25, 2024 







