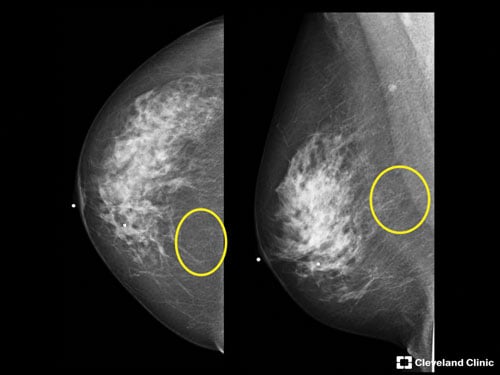
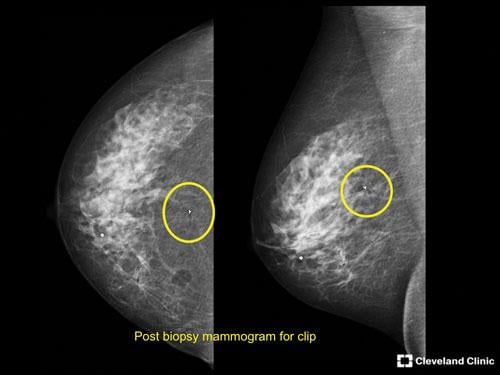
This image shows a 52-year-old patient with benign calcifications in her pre-stereotactic breast biopsy screening.
Recently, I was invited to participate in a roundtable discussion focused on uncovering the challenges and inefficiencies associated with stereotactic breast biopsies. In preparation, my colleagues and I spent a good deal of time reviewing patient case studies to identify a few that would best illustrate the issues related to this diagnostic procedure. As a board certified radiologist and associate director of breast imaging at the Cleveland Clinic, I have performed countless stereotactic breast biopsies on women over the past few years, and while every patient situation is certainly unique, the challenges we run into while performing these procedures remain consistent, time after time.
An Outdated Procedure
In a typical scenario, a patient will arrive for a breast biopsy feeling — understandably — anxious and concerned about the procedure itself, and that her results are going to reveal a cancer diagnosis. Upon arrival in the procedure room, which may also be the only room in the facility with a mammography system, the technologists work with the patient to determine the best possible position to target the area of concern. More often than not, those techs are forced to get creative, especially when the calcifications are in a hard-to-reach location or a patient has physical challenges that make maneuvering around a prone or upright biopsy system even more difficult. Once the patient is in position, she is required to stay still, typically with the needle in place, until the radiologist obtains and verifies a sample to ensure the specimen includes a sampling of the targeted abnormality as seen on the initial mammogram. If the sample is not sufficient, the process repeats itself until the verification proves positive.
During a time when physicians and institutions are expected to deliver high-quality care while simultaneously operating with patient experience, cost and efficiency in mind, the current state of stereotactic breast biopsy remains an outdated and problematic procedure for a number of reasons. Valuable time, if even only minutes, is often lost in the tissue sample verification process since a great deal of facilities lack technology allowing the team to verify samples in the procedure room. Patients fearing the worst, and often struggling to remain calm in an undesirable situation, may be required to remain still in an uncomfortable position for a lengthy period of time — made even longer by the added time spent waiting for the verification of core samples. Patients in the waiting room, awaiting their own breast biopsies, experience longer wait times and most likely, increasing anxiety. The overall time loss and added patient stress trigger a series of challenges for technologists, radiologists, pathologists and administrators across the health system.
Focus on Improvements
As my colleagues and I prepared for the aforementioned roundtable discussion with those inefficiencies in mind, we selected six case studies that represented a diverse mix of patients with a wide range of mammogram results and biopsy experiences. From a 77-year-old woman with multiple anterior and posterior calcifications, to a 55-year-old with known cancer and high anxiety, to a 49-year-old woman with ductal carcinoma in situ (DCIS) and past neck and knee surgeries that caused difficulty in getting positioned on a prone table — each situation further reinforced the delicate nature of this common procedure and the need for improvements that will make a positive impact on both the patient and the health system.
The most urgent need, in my opinion, is a more intense focus on patient comfort — not only by the techs and radiologists caring for the patients before, during and after the breast biopsy, but also by the research and development teams at the major manufacturers behind the technology we currently use to perform stereotactic breast biopsies. Healthcare systems should take extra steps to ensure their breast centers are designed with care to ensure a welcoming and practical environment for a diverse population of patients. That means creating procedure rooms large enough for the patient and staff to maneuver comfortably and accommodate positioning challenges that present themselves in nearly every breast biopsy procedure. Rooms must also have ample storage for the necessary equipment we need available — such as pillows, sheets and cushions to saline bags and molding dough. Many of us rely on these items to increase patient comfort and better access to hard-to-reach target areas.
Consider the Challenges
When designing new breast biopsy technology and equipment, I urge R&D teams to consider those of us on the front lines and the challenges we face when trying to deliver a positive patient experience during a procedure. No matter the technological advances the future will hopefully bring, biopsies will always cause women anxiety, discomfort and fear. Anyone who has performed a breast biopsy has encountered a number of scenarios throughout the procedure that underscore the need for better ways to modify the environment for patients with special circumstances. For example, patients with physical limitations or medical needs, such as a colostomy bag or oxygen tank, often have trouble positioning on the table. We all have also encountered the patient whose anxiety and apprehension can delay the procedure.
When it comes to technology, the gap between diagnostic screening technology, such as tomosynthesis, and the existing methods to analyze and verify tissue samples, remains greater than it should be. This can cause difficulty for those of us trying to assess concordance of pathology results with imaging findings. Finally, for those facilities that do not have the ability to image the specimen in the procedure room, the amount of time spent traveling outside the procedure room to complete this task is on average an additional three to five minutes per procedure. This could be trimmed significantly if there was a better way to conduct the imaging in the same room where the breast biopsy is performed.
In a time when patient satisfaction and facility efficiency are paramount, the current state of stereotactic breast biopsy presents challenges for many professionals who are tasked with evaluating their facilities’ workflow and overall bottom line. Also, this is not to mention those of us who spend our days interacting with the patients who rely on us to deliver a superior level of care during a difficult time in their lives. There is an urgent need for a better system that could improve the stereotactic breast biopsy procedure for the patient, doctor and technologist. Hopefully the manufacturers will respond and change is in our future.
Editor’s note: You can view the Roundtable Discussion at the Cleveland Clinic, featuring Laura Shepardson, M.D., Susan Miller, M.D., and technologists Cynthia Miller and Stacy Veri at http://www.itnonline.com/roundtable/stereotactic-breast-imaging.
Laura Shepardson, M.D., is the associate director of breast imaging at the Cleveland Clinic. She attended Cornell University, received her master’s degree in epidemiology and biostatistics from Case Western Reserve University, then worked for the Cleveland VA Medical Center as a biostatistician before enrolling in Case Western Reserve School of Medicine. She subsequently completed her residency in diagnostic radiology and fellowship in breast imaging at the Cleveland Clinic in 2008. Shepardson was appointed the Imaging Institute patient experience officer in 2009, and the associate director of breast imaging in 2010. Shepardson currently serves on multiple breast cancer and breast imaging committees, both at the local and national levels.

 April 24, 2024
April 24, 2024