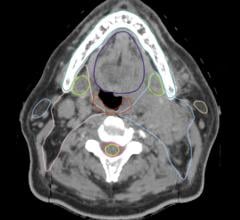
This is a 3-D endoluminal view from a CT colonography supine scan shows a sessile polyp colored red by the CAD software.
As an abdominal radiologist, I have integrated the advances of virtual colonoscopy (VC) research into our daily clinical practice. I would like to describe some of those experiences and clinical advances regarding the important topic of colorectal cancer screening using VC.
Colorectal cancer is the second most common cause of cancer deaths in the United States and many deaths could be prevented. The American Cancer Society recommends that colorectal cancer (CRC) screening start at 50 years of age for average risk individuals. The goal of screening is to detect both cancers and premalignant polyps (adenomas), which are precursors to cancer.
Virtual colonoscopy, also known as computed tomography colonography (CTC), is a low radiation dose CT scan of the cleansed and gas-distended colon designed to detect polyps and masses. It has some advantages over conventional optical colonoscopy in that it is minimally invasive (only a small tube is used to insufflate the colon with carbon dioxide gas or room air), it does not require sedation (thus it can be performed in an outpatient setting in only a few minutes and patients can return to work the same day – as did President Obama when he underwent a virtual colonoscopy[1]) and can be done even following an incomplete optical colonoscopy.
Virtual colonoscopy has undergone several years of development, and validation and clinical trials have shown that this test can reliably detect polyps and masses in the colon. Virtual colonoscopy for CRC screening has been endorsed by several organizations, including the American Cancer Society.
Recent Advances and Areas of Research
Some areas of immediate impact to the practice of virtual colonoscopy include fast novel visualization software for interpretation, new fast CT scanners with ultra-low radiation doses for VC, U.S. Food and Drug Administration (FDA)-approved software for computer-aided detection (CAD) of polyps on VC and research on “prepless” VC.
VC interpretation requires specialized training using dedicated visualization software to show the colonic surface in 3-D fly-through and multiplanar reconstructed images. Several vendors have alternate display options that show the colon as a flat surface for fast inspection. They have various names, such as “virtual pathology,” “virtual dissection,” “filet view,” “cube view” and others. We usually “fly through” the colon four times, forwards and backwards when reading the supine and prone views. Using an unraveled view might speed up the interpretation and can be integrated into CAD software discussed below.
The concerns raised regarding radiation dose in CT in general are not applicable to virtual colonoscopy. The doses we now use in VC are similar to those to which the general U.S. population is exposed from nonmedical sources in one year.
New dose reduction algorithms also have helped. I routinely use 15-30 mA, resulting in exams of 2-4 mSv (supine and prone combined dose). The scans are quite fast, allowing acquisition of each series in a breath-hold of 10 seconds or less.
The majority of errors in interpretation have been shown to be polyps which were missed, but can be found on VC in retrospect. Also, the exam is normally interpreted using both 3-D and 2-D methods, yet the review of the 2-D images for polyps can be a tedious task. Novices are more prone to make errors (both misses and false positive interpretations) and require long interpretation times.
For these reasons, the use of CAD software to improve reader performance is extremely valuable, both for the novice and experienced readers. Since software for CAD is now FDA-approved, we have integrated CAD into routine VC interpretation.
Early Computer-Aided Detection for VC
Computers can segment the colon from the remainder of the abdominal structures on the CT scan and analyze the shape of the mucosal surface of the colon to find polyps and masses (see image). False positive reduction algorithms then eliminate many mimics of polyps, such as retained stool, colonic folds and the rectal tube.
CAD software should be “trained” and “tested” on different cohorts. The first step is “stand-alone” testing, meaning how well does the CAD find polyps known to be present as compared to optical colonoscopy or to multiple experts’ reading of the CTC and how many false positive marks are generated. The CAD sensitivity, similar to CTC reading clinically, is stratified by polyp sizes (6-9 mm or >10 mm) and by polyp histology (adenomas vs. other histologies with no malignant potential). Human readers may opt to accept or reject CAD marks; therefore, in order to claim efficacy in CRC detection, clinical observer trials are needed to demonstrate improved exam performance.
CAD Clinical Observer Trials
In the first large clinical observer trial using CAD to read virtual colonoscopy, published in Radiology, CAD was shown to improve overall reader performance.[2] This study was based on the interpretation of 100 screening CTC exams interpreted both without and with CAD by 19 readers drawn from both academic and private practice settings.
The readers used VeraLook software by iCAD in a “second reader mode,” in which the case was read separately without CAD and subsequently with CAD assistance. This is the most rigorously conducted CAD trial to date, particularly in the methodology used to define the standard of truth using comparison to optical colonoscopy when available and a team of experts who had to agree on polyp location, size and pixel-by-pixel painting of every single polyp on CTC.
This study showed that the sensitivity for detecting polyps >6 mm improved by 11.8% and 19.9% for polyps 6-9 mm. Specificity decreased by only 2.7%, and reading time increased by 4.5 minutes. (Currently, after more experience with CAD, I find it only adds a couple of minutes to my read[3]).
In stand-alone testing, the CAD was 94.4% sensitive for patients with at least one polyp >10 mm and 90.2% sensitive for patients with small polyps between 6 and 10 mm. The average number of false marks for all cases with positive findings was 5.07 and 4.08 for negative cases.
This study concluded that the use of CAD results in a significant improvement in overall reader performance. The CAD system improves reader sensitivity when measured at the segment, patient and polyp levels for small polyps and adenomas. The average reader sensitivity improvement with CAD was the most for small adenomas.
Use of this CAD system also reduces specificity and increases reading time, but the reduction in specificity is small. My personal perspective is that CAD will perform even better in clinical practice settings, given the additional experience we have in using it since the clinical trial was conducted.
Limited Colon Cleansing
What people dislike most about colorectal cancer screening in general is the colon catharsis. If virtual colonoscopy could be performed without a preparation, that would be a major advance.
In fact, there has been a body of literature since 2004 showing the feasibility of reducing or eliminating the colon preparation. While this is still not recommended for routine virtual colonoscopy, a limited preparation combined with tagging of the residual fluid and stool can produce a diagnostic-quality exam. Active research is being performed to combine such limited or non-cathartic studies with CAD as well.
Future Outlook for VC
In July 2011, the Center for Disease Control released new figures showing that colorectal cancer screening has decreased the number of cancer deaths from 2003 to 2007. Yet the director, Dr. Thomas R. Frieden, emphasized that, “The momentum is slowing and numbers appear to be leveling off.”
I think the public and the medical establishment should recognize the enormous potential of virtual colonoscopy to improve CRC screening compliance. The advent of new software programs and particularly computer-aided detection can help radiologists confidently initiate a CTC screening program and render accurate interpretations. With the increase in reimbursement for CTC and more radiologists learning to interpret the exam, I expect CAD will become an integral component of CTC interpretation.
Abraham H. Dachman, M.D., FACR, is professor of radiology at the University of Chicago and has been conducting research on virtual colonoscopy since 1994. He is author of the first text on the subject, “The Atlas of Virtual Colonoscopy,” and the recently released second edition. He has authored more than 80 publications or book chapters on CTC. He participated in CAD software development at the University of Chicago in collaboration with computer scientists and is co-patent holder on the product developed. He is currently studying the clinical features of observer CAD false negative and false positive interpretations.
References:
1. www.auntminnie.com/index.aspx?sec=sup&sub=vco&pag=dis&ItemID=89674
2. Dachman AH, Obuchowski NA, Hoffmeister JW, Hinshaw LJ, Frew MI, Van Uitert, RL Summers RM, Hillman BJ. “Impact of computer aided detection for CT colonography in a multireader, multicase trial.” Radiology. 2010; 256:827-835.
3. Dachman AH, Laghi A (eds). “Atlas of Virtual Colonoscopy, 2nd edition.” Springer-Verlag, Inc. New York, N.Y. January 2011.

 April 16, 2024
April 16, 2024