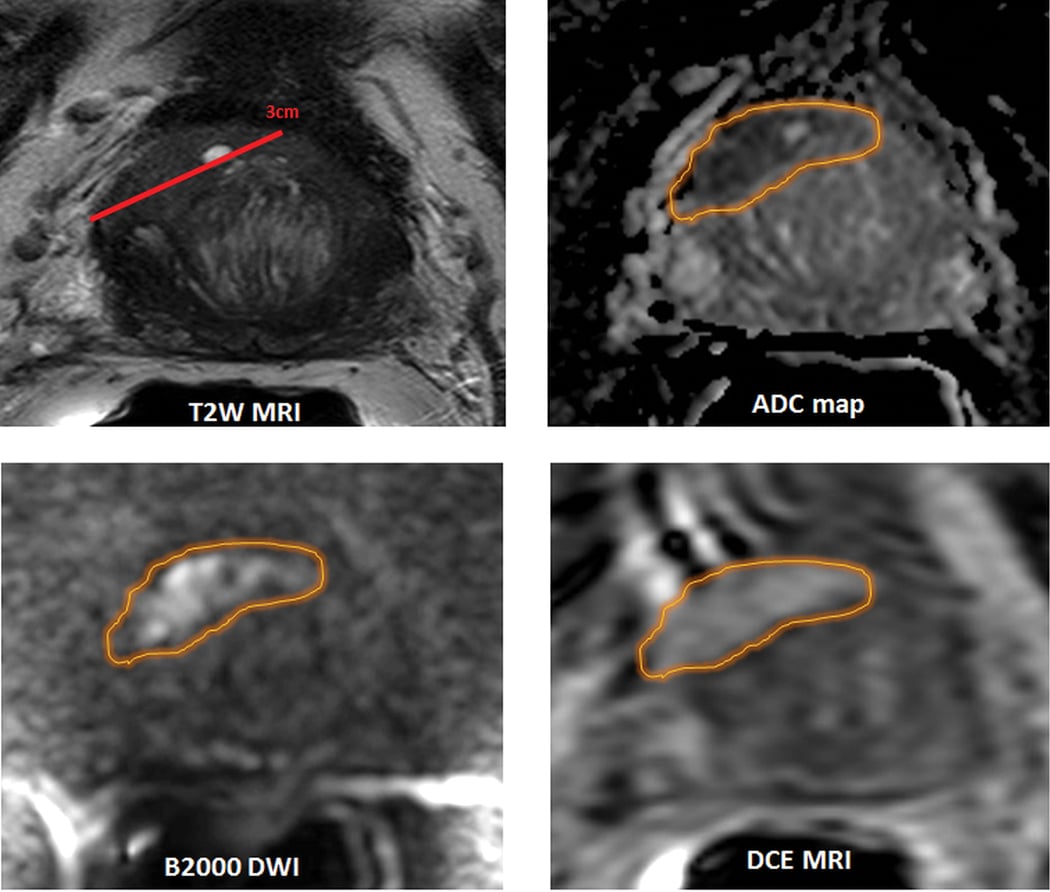
Multiparametric MRI (MpMRI) has proved helpful in enhancing biopsy sampling for prostate cancer when combined with ultrasound.
While prostate cancer is one of the most common cancers among American men — the third leading cause of cancer deaths in that group according to American Cancer Society statistics — it is a complex condition that encompasses a broad range of disease and numerous stages. As a result, imaging it for detection and management purposes has traditionally been difficult. New technologies have emerged in the last several years, however, that appear promising for improvements in these areas. Several of these technologies were highlighted during an educational session at the 2016 annual meeting of the Radiological Society of North America (RSNA) in November in Chicago.
The Status of Prostate Cancer Imaging
The majority of imaging research and advancements related to prostate cancer have centered around diagnosis and detection according to Peter Choyke, M.D., FACR, program director, molecular imaging program, senior investigator, head, imaging section, Center for Cancer Research at the National Institutes of Health (NIH). Issues of concern here include:
• Risk assessment
• Biopsy guidance
• Staging
• Surveillance
• Focal therapy
The next frontier, where researchers are beginning to make strides, Choyke said, is in detecting and treating recurrent prostate cancer. Issues being studied in this field include:
• Locating recurring cancer
• Biopsy guidance
• Therapy direction
As for metastatic disease, Choyke said advanced imaging work is just beginning in this area. Prostate-specific antigen (PSA) screening has appeared to lower metastatic disease rates (and by extension mortality rates), but currently the U.S. Preventive Services Task Force (USPSTF) recommends against it, saying the benefits are outweighed by the potential harms of overdiagnosis and treatment. As a result, more patients are again starting to present with metastatic disease. “This is the area that leads directly to death, so this would have a huge impact,” Choyke said. Imaging research related to detection and treatment of metastatic disease is centered on:
• Imaging sensitivity
• Disease response
• Castration
Multiparametric MRI
Magnetic resonance imaging (MRI) has proven to be one of the more effective imaging modalities for prostate cancer, helping improve localization and guidance of biopsies, especially for anterior cancers. According to Choyke, T1 and T2 stage disease that is confined to the prostate is easily detectable on MRI, while extra-prostatic disease (T3 and T4) are harder to visualize.
Because of the disease’s variable nature, researchers and clinicians in recent years have started using multiparametric MRI (mpMRI), combining functional and anatomic imaging via several different sequences to provide a more complete picture. mpMRI exams typically include T2-weighted imaging for anatomy, diffusion weighted imaging (DWI) for cellularity and dynamic contrast-enhanced MRI (DCE-MRI) for vascularity.
A number of clinical studies have assessed the effectiveness of mpMRI for prostate cancer, and have determined it is the best noninvasive alternative for tumor detection. One study, published in the Journal of Magnetic Resonance Imaging last July, looked to assess the performance of mpMRI as described in version two of the Prostate Imaging Reporting and Data System (PI-RADS). The research team found that mpMRI achieved 91 percent sensitivity in detecting clinically significant index lesions and 63 percent for all lesions across all readers.1
There has also been success in combining mpMRI with ultrasound to improve biopsy sampling. A study from the January 2015 Journal of the American Medical Association (JAMA) compared mpMRI/ultrasound-guided biopsy with standard biopsy; the image-guided biopsy diagnosed 30 more high-risk cancers than standard biopsy, and also diagnosed 17 percent fewer low-risk cancers, suggesting that targeted biopsies can help reduce overdiagnosis while still catching more developed disease.2
Challenges with mpMRI. As beneficial as multiparametric MRI has proven for visualizing prostate cancer, it does still have its challenges, according to Baris Turkbey, M.D., associate research physician, Molecular Imaging Program at National Cancer Institute’s Center for Cancer Research. For one, the technique does not entirely eliminate the variation seen in prostate cancer — Turkbey shared the experience of one patient who had three mpMRI scans in a three-month period at three different hospitals and came away with three different results.
Turkbey also noted that unlike other MRI exams, the type of coil that is needed can vary for prostate exams. “Some say a phased array coil is good and some say an endorectal coil is good,” he noted. If you do use a coil, you must decide what to use inside the coil, where again, Turkbey noted there has been great variation.
Apart from cost — Turkbey told his RSNA audience that mpMRI is still a fairly expensive procedure — perhaps the most significant obstacle is that its effectiveness is limited in local staging. A study from the August 2016 European Urology journal found that mpMRI achieved only 57 percent sensitivity (but 91 percent specificity) with T3 disease.3 Turkbey said that overall, mpMRI still misses approximately 10 percent of clinically significant prostate cancers.
CAD and mpMRI. One solution that may help improve the capabilities of mpMRI is computer-aided detection (CAD), which Turkbey briefly discussed at RSNA. According to one study he cited, adding CAD to the initial scan improved sensitivity 8.4 percent for index lesions for all readers. The research team also saw a 16 percent reduction in further unnecessary biopsies as a result.
Hyperpolarized C-13 MR Molecular Imaging of Prostate Cancer. Some work is also being done to increase the sensitivity of MRI through hyperpolarization of pyruvate acid. When injected into the body, it is normally converted to carbon dioxide or alanine — but in the presence of aggressive cancer it converts into lactate, according to Daniel Vigneron, Ph.D., professor and director of the Hyperpolarized MRI Technology Resource Center at the University of California-San Francisco. A phase 1 safety and feasibility clinical trial of 31 patients found that tracing these enzymatic activity changes allowed a functional look at prostate cancer metabolism.
PET Imaging of Prostate Cancer
Nuclear imaging, in particular positron emission tomography (PET), has offered another promising avenue, with several classes of imaging agents developed for prostate cancer applications. The majority of PET agents track uptake of prostate-specific membrane antigen (PSMA), a protein that tends to be associated with aggressive prostate cancers and also acts as a marker of androgen signaling.
Monitoring PSMA uptake can serve several purposes in prostate cancer detection and treatment, according to Martin Pomper, M.D., Ph.D., Henry N. Wagner Jr., M.D., Professor of Radiology at Johns Hopkins University. Some ways that it has been used include:
• Selecting candidates for active surveillance;
• Pre-surgical staging in patients at risk of occult metastatic disease;
• Direct therapy when patients experience PSA recurrence after failing local therapy; and
• General therapeutic monitoring.
Pomper noted that PSA cannot provide information related to the location or aggressiveness of cancer, and that conventional imaging has performed poorly for prognosis in castration-resistant prostate cancer (CRPC), further supporting the use of molecular imaging.
Fludeoxyglucose (F-18) is the most commonly used PET agent for prostate imaging in the United States. It was predated by carbon-11, but that molecule features a three-minute half-life, making it not clinically translatable, according to Pomper. Conversely, F-18 features a longer half-life, making it easier to transport and mass produce domestically. “It also features a short positron path range, so you get a much crisper image,” Pomper said during his RSNA presentation.
PET/MRI
While PET and MRI each offer distinct advantages in prostate cancer imaging, many in the industry believe that combining the two can provide even greater benefits. Choyke noted that radiologists and researchers have been looking for the “killer application” for PET/MR since its inception, and prostate imaging has offered the most promising avenue thus far.
“MRI is an important part of prostate cancer management, but numerous new PET agents provide high sensitivity and specificity for prostate imaging, so it makes sense to combine the two,” he told the RSNA audience.
The real question, he said, is whether enough patients need simultaneous PET/MR scans to justify the $5-7 million price tag of these machines.
Choyke further supported the utility of PET/MR for prostate cancer imaging by comparing it to PET/CT (computed tomography). One study published the previous January in the Journal of Nuclear Medicine found the two combination modalities performed equally well in lesion detection and image quality. The researchers did find, however, that PET/MRI was more accurate for anatomic lesion allocation within the prostate, which could have implications for biopsy planning.4
One of the advantages of PET/MRI, Choyke said, is that with the full-body scanning capabilities of today’s MRI machines, it is possible to overlay PET images on top of the MRI scans for improved visualization. The combined modality has also demonstrated improved anatomic localization of recurrent lesions.
Perhaps most importantly, however, Choyke said that PET/MRI has allowed a more sophisticated PSMA scan, which he said is highly accurate for early metastatic disease. “We’ve been able to look at both primary tumors and recurrent cancers,” he told the RSNA audience. There is limited data beyond this for PET/MR with metastatic disease, but more studies are ongoing and on the horizon.
Challenges of PET/MRI. For hospitals looking to implement PET/MR for prostate cancer imaging, Choyke said the No. 1 challenge will be establishing a new workflow. “It is difficult to find technologists that are skilled in both PET and MRI,” he told his audience, “so you need two actively involved staff members.” This means that extensive training will be required for any kind of implementation, taxing critical resources of time and money. Further complicating the financial side, Choyke noted that the pay scale for technologists is often not adaptive to combined modalities.
More than training differences, however, Choyke said that the culture of the two technologies is very different. “MRI typically is a modality that needs to be monitored very closely for image quality accounting for motion,” he explained, whereas PET imaging does not often require rescanning. From a safety perspective, MRI technologists are not used to working with radioactivity, while PET technologists may not be aware of the zoned safety approach required for MRI scans.
“It is clearly a step forward in technology and the evolution of hybrid imaging,” Choyke said of PET/MR, “but the economic argument will have to be made for it if it’s going to be sustainable.”
References
1. Greer, M.D., et al. “Accuracy and Agreement of PIRADSv2 for Prostate Cancer mpMRI: A Multireader Study,” Journal of Magnetic Resonance Imaging. Published July 8, 2016. DOI: 10.1002/jmri.25372
2. Siddiqui, M.M., Rais-Bahrami, S., Turkbey, B., et al. “Comparison of MR/Ultrasound Fusion-Guided Biopsy With Ultrasound-Guided Biopsy for the Diagnosis of Prostate Cancer,” JAMA. Published Jan. 27, 2015. doi:10.1001/jama.2014.17942
3. De Rooij, M., Jamoen, E.H.J., Witjes, A., Barentsz, J.O., et al. “Accuracy of Magnetic Resonance Imaging for Local Staging of Prostate Cancer: A Diagnostic Meta-analysis,” European Urology. Published online Aug. 1, 2016. DOI: 10.1016/j.eururo.2015.07.029
4. Spick, C., Herrmann, K., Czernin, J., “18F-FDG PET/CT and PET/MRI Perform Equally Well in Cancer: Evidence from Studies on More Than 2,300 Patients,” Journal of Nuclear Medicine. Published Jan. 21, 2016. doi:10.2967/jnumed.115.158808

 April 18, 2024
April 18, 2024