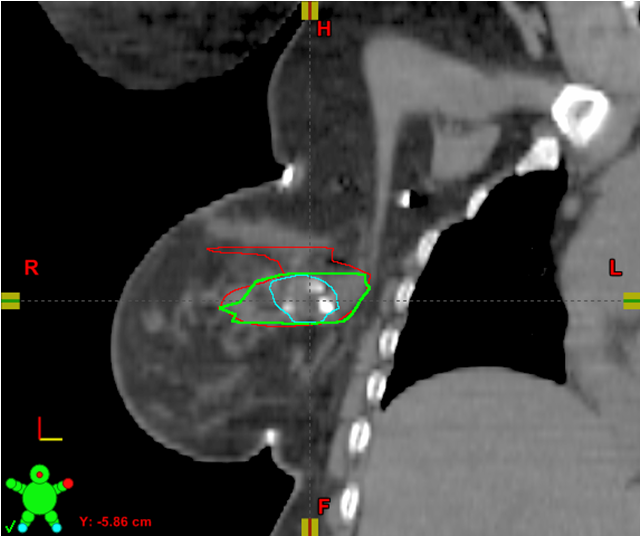
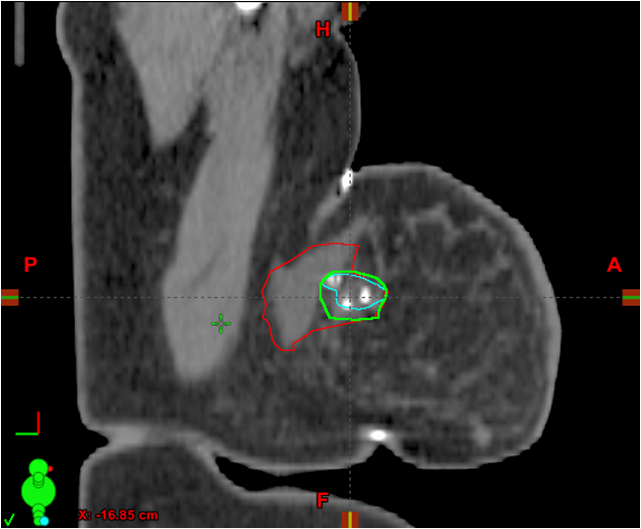
These CT images show placement of a 3-D fixed array implanted fiducial (3-D marker) at the time of oncoplastic tumor resection. The original LCTV (LCTVo) was retrospectively re-contoured by the radiation oncologist (LCTVro) and breast surgeon (LCTVbs). Thereafter, both re-contours were combined to create the collaborative LCTV (LCTVc), which required agreement of both the radiation oncologist and breast surgeon. Volume differences between the original LCTV (LCTVo) and the collaborative LCTVc were then evaluated, and demonstrated a mean and median reduction in LCTV.
Radiation planning for breast cancer relies on accurate delineation of the post-lumpectomy target volume as identified on non-contrast axial computed tomography (CT). Visible seroma, surgical clips and adjacent tissue are typically included when contouring the lumpectomy clinical target volume for radiation treatment. Radiation oncologists and treatment planners face challenges that can make clear delineation of the lumpectomy cavity problematic.
These challenges include:
• Growing use of oncoplastic surgery (OPS). OPS represents a tremendous advance in its capacity to preserve the pre-surgical appearance of the patient’s breast. However, extensive surgical rearrangement of breast tissues creates seromas and results in vascular clip placement in areas that may not be not associated with the actual tumor site, resulting in unnecessarily large seroma-based target volumes.
• Patients with dense breasts. Dense breast tissue, which is common in premenopausal patients, can make identification of the lumpectomy cavity site very difficult, as there is often no clear seroma or lumpectomy site visible.
To compensate for the uncertainties these challenges can cause, planners will often designate a large area of the breast for treatment to ensure the entire tumor site is included. This is a prudent approach from a cancer control standpoint, but increases the volume of normal breast tissue irradiated with boost or partial breast treatment. As the target volume in the breast becomes larger, the radiation exposure to the heart, lungs and chest wall increases as does the potential deleterious effect on cosmetic appearance.
I conducted a preliminary study with breast surgeon Cary Kaufman, M.D., associate clinical professor of surgery at the University of Washington and the medical director of the Bellingham Regional Breast Center, on a promising approach for addressing these issues. We examined the use of an implanted device (BioZorb 3-D bioabsorbable marker, Focal Therapeutics) which is sutured to the tumor site and marks the true lumpectomy cavity in three dimensions using surgical clips arranged in a fixed 3-D array. The clips are easily identifiable on most imaging modalities including diagnostic CT, cone beam CT and kilovoltage (kVp) imaging systems. The main body of the device is made of a bioabsorbable material and is reabsorbed over the course of a year to 18 months while the clips remain in place indefinitely.
The device is specifically placed in the tumor site. It aids in overcoming the challenges posed by OPS, dense breasts, migrating clips and misleading seromas. With more certainty about where to target the radiation, radiation oncologists and treatment planners can devise smaller, more accurate target volumes, thereby reducing the dose to normal tissue and organs, and potentially leading to better cosmetic results.
Do these attributes turn out to be true in practice? We reviewed of our first 10 patients who underwent placement of the 3-D implant at the time of OPS. We found the device could reduce radiation target volume by approximately 60 percent. The study was presented at the annual conference of the American Society for Radiation Oncology (ASTRO) in 2016.
The following sections discuss how the study was conducted, our conclusions beyond the target volume reduction, and the broad implications this device has for our field. (Editor’s note: You can watch William Hall, M.D., talk more about this study in the video “Study on 3-D Marker That Reduces Radiation Target Volumes” at http://bit.ly/2i2BcX9.)
Study of the 3-D Implant
Our initial study of the implant involved our first 10 patients who had the device placed during their lumpectomy surgery. All of the patients had received OPS as part of their procedure. In the first phase of the study, patients received radiotherapy with standard target delineation techniques and were contoured by myself or one of my partners. In this phase, there was no collaboration between the surgeon and radiation oncologists. The volumes devised in the first phase were those used for patient treatment. In the next phase, Kaufman and I retrospectively and separately re-contoured the lumpectomy cavity volume (LCTV) for each patient with the implant informing our contour volume. We then combined our LCTVs to create a collaborative LCTV that we mutually agreed upon. The collaborative LCTV was substantially smaller than the target volume based on standard targeting methods.
How does the 3-D implant help us address modern challenges in lumpectomy cavity target delineation?
• Challenges caused by OPS. The seromas created by mobilizing tissue for OPS can distract treatment planners who rely on seroma formation to guide them to the tumor site. If the planners look for the implant instead of seromas on their CT scan, they can easily see exactly where the tumor site is located.
• Challenges caused by dense breasts. Breast density is not an impediment to seeing the implant on the planning CT image. Also of note is the fact many patients with dense breasts are younger women with cancers that are at high risk of recurrence, so accurately treating their tumor site is extremely important. The implant is a strong tool in that regard.
• Challenges caused by migrating clips and non-local seromas. The implant replaces unstable or unreliable markers with one that is firmly attached to the tumor site.
How can the 3-D implant benefit breast cancer patients and their treatment team?
• Potentially improved cosmetic outcomes. Hypothetically speaking, reduced target volumes should translate to less radiation exposure to healthy tissue surrounding the lumpectomy site. That in turn should mean less radiation fibrosis formation in the breast and thus improved cosmetic outcomes. Others have reported additional advantages from a cosmetic standpoint. The implant helps fill the gap left by the tumor removal. Without the implant, the healing breast often collapses into that space, creating a lumpectomy divot. The implant helps solve the problem for many patients. For others, it makes it less severe. With more patients requesting OPS, the gap can also be mitigated with tissue mobilization. Having the implant in the gap reduces the amount of mobilization that needs to be performed. In addition, some researchers have reported that the implant serves as a scaffolding for OPS — that is, a stable framework to which mobilized tissue can be attached.
• Collaborative tool. The device aids the necessary communication between breast surgeon and radiation oncologist about where the tumor site is located. The device can be clearly seen on imaging equipment and there is no question that the device represents where the “true lumpectomy cavity” is located.
• Increased eligibility for APBI. Results from the National Surgical Adjuvant Breast and Bowel Project (NSABP) Protocol B39, which looked at accelerated partial breast radiation (APBI) vs. whole breast radiation, are pending. The B39 protocol establishes constraints of less than 60 percent of the whole breast reference volume receiving 50 percent of the prescribed dose and less than 35 percent of the whole breast reference volume receiving the prescribed dose. That is a high bar to meet. Assuming that further study confirms that use of the implant dependably reduces LCTV, we think its use may also increase the number of women who qualify for external beam APBI.
• Smaller boost volumes for patients receiving WBI. Those patients who must receive whole breast radiation (WBI) often receive a boost treatment that is a crucial part of their radiotherapy. With ther implant, we should be able to reduce those boost volumes
because we’ll know exactly where to target the treatment.
• More efficient use of physicians and therapist time. In my practice, the uncertainty with the use of standard targeting methods leads to more time doing the actual treatment. Using MV ports or cone beam CTs to verify beam position when targeting a lumpectomy cavity for APBI or breast boost can be problematic with difficulty visualizing the lumpectomy cavity on cone beam CT and multiple pretreatment reports. That time is saved when the 3-D implant is used because we know exactly where to aim. Put simply, increased certainty equals increased efficiency.
Future Outlook
Our study suggests that the process of delineating the post-lumpectomy radiation target volume has taken a step forward with the advent of the BioZorb 3-D implant. More study of this device with larger populations is certainly warranted. Several other studies and initial experiences have already been conducted and reported to date. This research has consistently shown substantial reductions in radiation target volumes, more precise treatment and making more women eligible for shorter, more convenient courses of radiation. We have seen no significant downsides to using the implant thus far. We believe there is enough evidence on hand to recommend the implant’s routine use.
William Hall, M.D., is a radiation oncologist in the Department of Radiation Oncology at PeaceHealth St. Joseph Medical Center in Bellingham, Wash.

 April 18, 2024
April 18, 2024