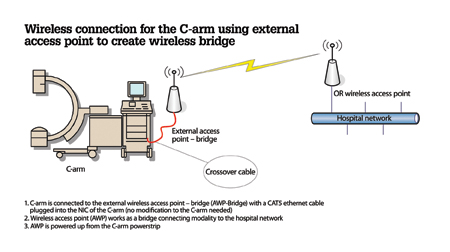
Appendix 2: Network engineers helped develop a working prototype for a Wi-Fi access point as a step to implementing wireless connectivity for modalities such as the C-arm shown in this sample diagram.
Broward Health Medical Center (BHMC) is a 716-bed, Level I trauma center located in downtown Fort Lauderdale, Fla., serving Broward County residents since 1938. Its radiology department is a comprehensive diagnostic imaging center averaging more than 700 studies per day. BHMC’s radiology picture archiving and communications system (PACS) was implemented in May 2005, just prior to a major expansion of the emergency department (ED), critical care units, operating room (OR) and outpatient services.
At that time, the major focus of the PACS implementation was on making image workflow not only filmless, but also paperless. To achieve this goal and to provide ED physicians with an electronic form of communication with radiologists, a set of business rules were implemented.
Taking a Proactive Approach
To achieve sustainable excellence in the quality and safety of healthcare, the radiology department took a proactive approach to identify bottlenecks in study flows and streamline processes at every stage of imaging studies, from order entry to report posting. Our ultimate goal was to provide ordering physicians with radiologists’ reports in time to support a clinical diagnosis in an acute setting. This goal aligns with the strategic initiatives of our organization to achieve meaningful use (MU) of radiology reports and allow physicians to initiate treatment more promptly.
Process Improvement (PI) Methodology
The radiology department had a set of policies and procedures (P&P) that set the rules and sequences of steps that needed to be taken for a variety of processes. However, the departmental P&Ps did not depict or account for the concurrent processes that take place in the real world. Previously, several attempts had been made to model radiology processes by using Visio diagrams and unified modeling language (UML) tools (see Appendix 1), but no quantification methods were used to predict the maximum sustainable throughput of the processes.
Our information systems management team offered to assist us by using ICOR (inputs, outputs, controls and resources) as a comprehensive methodology for process improvement (PI) in healthcare settings. It allows processes to be broken down into simple, manageable and more easily understandable units. In addition, process mapping provides a common framework and discipline in language, allowing a systematic way of working for the PI team. Complex, multilayered interactions and business rules can be represented in a logical, highly visible and objective way.
As a part of the brainstorming phase, “what if” scenarios were developed and maps of the process “as is” compared with the “to be” process. This approach illustrated well where issues existed and provided PI teams with a common decision-making framework.
Identifying Bottlenecks and Developing Solutions
Our PI team focused on the workflow of every modality, analyzing concurrent patient traffic, including conditions when the system is under stress due to unexpected staff shortage, modality outages or because of a high volume of studies. Being the largest trauma hospital in Broward County, we needed to re-engineer our processes to eliminate “single points of failure” and ensure the stability of our system under unexpected conditions.
Detailed process modeling gave us a comprehensive picture of the bottlenecks and highlighted the single points of failure that were not visible unless the system was stressed to its maximum capacity. As we analyzed processes, our brainstorming sessions yielded solutions that were tested and scored based on predicted effectiveness and implementation and maintenance costs without compromising patient safety. The solutions with the highest score were tested as prototypes and then implemented. Effectiveness of the solutions was re-examined and compared with the baseline results.
A Wireless Solution Saves Time for US
Granularity level of the ICOR analysis uncovered one reoccurring step in the ultrasound (US) portable process. Every time a technologist completed an ultrasound study, he or she needed to physically return to the department in order to upload the study to the PACS and receive an assignment for the next study. Due to the large physical size of our facility, a technologist could spend 15 minutes on the round trip from the patient to the department and back.
Wireless connectivity looked like a very promising way to cut down on such redundant routes for the US technologists. But our modalities did not support any add-on cards to implement wireless adapters.
Network engineers were invited to participate in a brainstorming session. We came up with a working prototype for a Wi-Fi access point, reprogrammed as a Wi-Fi bridge that extends Ethernet connectivity over the secured wireless network, which was totally transparent to the modality (see Appendix 2) and did not require any changes to our modalities.
After testing the signal strength and Wi-Fi throughput in all areas of the hospital, we realized this was a reliable alternative to a wired Ethernet connection. We connected our US machines to the Wi-Fi bridges and tested actual US image transfer from the modality to the PACS.
With about 30 to 40 portable ultrasound studies done daily, this implementation of Wi-Fi technology saved five to six productive hours or ¾ full-time equivalents (FTE) every day. This economical solution decreased turnaround time (TAT) for portable ultrasounds, which is especially critical for the ED, intensive care, and labor and delivery units. As a “side effect” bonus, we also reduced wait time and improved the TAT of ultrasound studies in our women’s center by redirecting that ¾ FTE to help US technologists in that area.
Dictation — Another Bottleneck and Solution
When we looked at our TAT for dictation, we initially felt we were in a good position because we had in-house transcriptionists who were very proficient and had a good rapport with our radiologists. However, when we analyzed the “what if” scenarios, we uncovered a potential bottleneck. If one of the two transcriptionists on the night or weekend shift called in sick, transcriptionist throughput decreased by 50 percent. When we looked at the actual attendance history, we saw that during the flu and holiday season, we did not have adequate resources to support the transcriptionists’ workload. We evaluated several options, including outsourcing transcription services to a larger company and introducing voice recognition services.
We contacted our peers and found a company that provides services to our clinical laboratory and pathology departments. We negotiated a contract with the company to have it hire our transcriptionists and provide us with consistent TAT of 15 minutes for STAT reports. Since we joined a large volume contract, the price per line was not much more than what we had been paying before, and we got high-quality services from the transcriptionists that used to work for us.
The positive outcome exceeded expectations. Our clinicians were able to see reports posted to an electronic medical record (EMR) in less time ever before.
Improvements for the ED
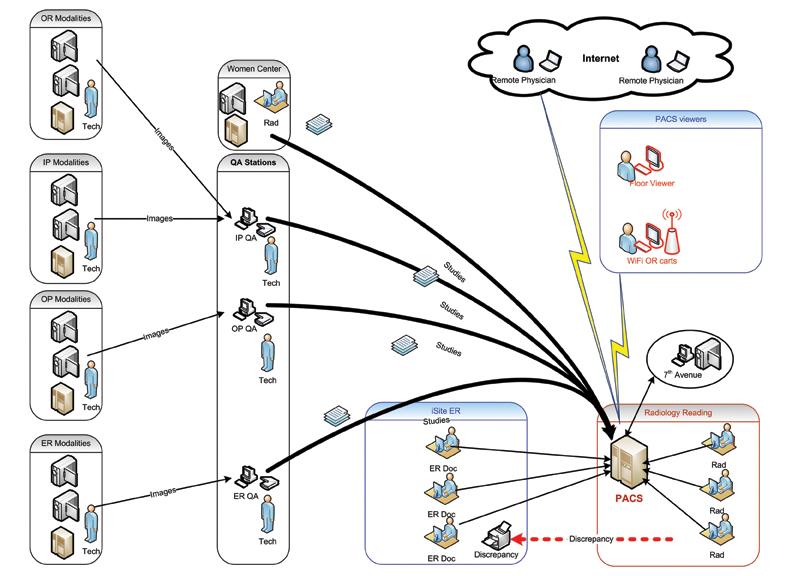
Based on the business rules established in 2005 for discrepancy reporting, an ED study flow was designed with a manual trigger that introduced a delay in the overall workflow. ED studies were sent to the ED physician viewing station for a “wet reading,” and the ED physician would record his or her impression before sending the study to the radiologist for reading. Quite often, the ED received the radiologist’s report after the patient had been discharged.
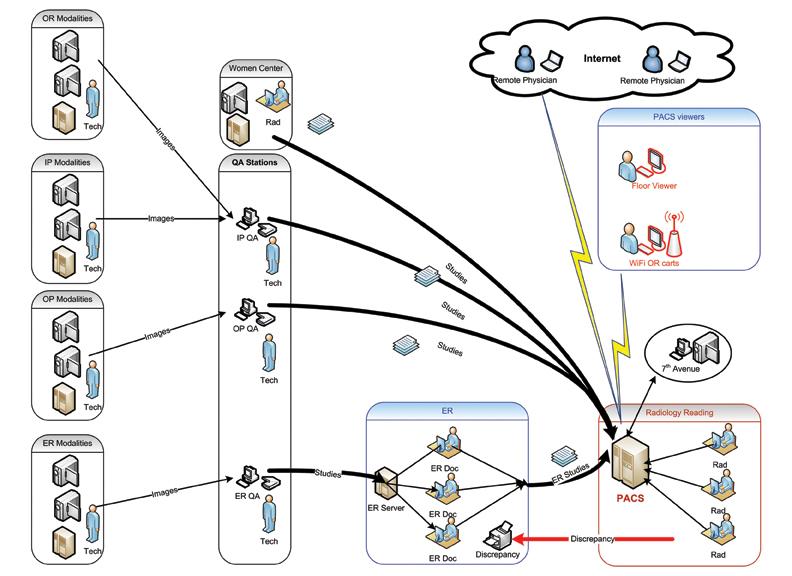
Our PI team got input from ED physicians and re-examined the existing process. Then we proposed a streamlined workflow that eliminated the human factor that had the potential to delay a study’s delivery to a radiologist. With the re-engineered process, studies are delivered to the radiologist and the ED physician simultaneously, without any artificial delay (see Appendices 3a and 3b).
This solution produced several positive outcomes. Besides significant reduction of TAT for ED studies, the ED had radiologist reports in almost all cases before the patient was discharged. This reduced the number of patients needing to be called back.
Streamlining the Women’s Health Center
Our state-of-the-art Lillian S. Wells Women’s Health Center provides a full range of services, including magnetic resonance imaging (MRI), ultrasound, mammography, US-guided biopsy, etc. Increased breast cancer awareness accelerated our search for the most streamlined and error-free processes.
Reading mammography requires the comparison of the most current results with previous studies, (US, MRI or mammograms), even if they are several years old. A large number of our female patients come with previous studies that have been done at local diagnostic centers or even abroad, which often creates data compatibility issues. This diverse environment required multiple viewers (mammography and MRI, computer-aided diagnosis [CAD], US and film viewers), and a complex paper-driven workflow. As a result, radiologists had to stop reading studies several times a day to have the film librarian hang a new set of studies and sort the paperwork accordingly.
On average, a radiologist spent almost 90 minutes a day waiting for studies to be set up on viewers. The film librarian spent hours of unproductive time waiting for the radiologists to be ready for them to hang a new batch of studies.
We focused our PI team on designing a unified process to bring all outside studies onto the mammography diagnostic workstation. The most apparent option was to import studies (from CDs and digitize film) into our PACS, but we also needed to manage the paperwork flow to accompany outside studies. To accomplish this we installed a DICOM images importer to automate the tedious process of extracting images from CDs. Next, we installed a film digitizer for mammography films and a paper scanner to scan the technologists’ worksheets.
The redesigned process includes importing prior (outside) studies into our PACS, scanning all paperwork into the corresponding study and making the exam complete once all the components are available on the PACS. The radiologist reads studies from the filtered worklist where all relative prior exams are automatically displayed on the screen for comparison. The film librarian can work independently from the radiologist scanning or importing the previous studies into the PACS. This workflow design yields one more benefit — patients are getting their CDs or films back before leaving the Women’s Center. No more lost CDs or films.
Re-Balancing the Workload
As we looked at the enterprise PACS, we realized that load balancing is essential to efficiently handle the radiologist’s workload. As a proof of concept, we moved one of Broward Health Medical Center’s PACS diagnostic stations to our sister hospital, Broward Health Imperial Point (BHIP). This gave a radiologist from BHIP an opportunity to help read studies for Broward Health Medical Center, especially when multiple trauma patients were being treated at BHMC.
A significant reduction of our TAT (1 hour) also gave us an opportunity to attract new business, such as providers of diagnostic imaging services for cruise line employees on ships coming to the port of Fort Lauderdale. In addition, we realized one more benefit — once we became an enterprise-based PACS in November 2011, we were able to route studies based on the radiologist’s specialty, providing the ordering physician with the highest quality reports.
More Wi-Fi Was the Next Step
After we realized how beneficial it is to “unleash” US modalities onto Wi-Fi, naturally our next step was to bring portable X-ray on Wi-Fi and convert them to digital radiography (DR). We contacted several vendors and evaluated a solution that allowed us to retrofit existing cassette-based portable X-ray machines into portable DR units.
According to data from Western Baptist Hospital in Paducah, Ky., “performing a portable chest study on the floor and transmitting it wirelessly represents a time savings of 10 to 15 minutes per patient, because techs no longer have to walk a cassette from the floor to the radiology department for processing.”[1] Based on our volume of portable studies (80 to 90 per day), if we were able to shave 10 minutes from the processing time, the difference would equate to nearly 15 hours per day or 5,500 hours annually.
Summary
Leading healthcare organizations may sustain a leadership position by constantly searching for process improvement. Multidisciplinary process improvement teams equipped with comprehensive information system management methodology can provide optimization solutions that will raise baselines to the next level of effectiveness, safety and improved clinical outcomes.
Just as the PACS installation at BHMC in 2005 became a baseline for our PI team, the process improvement initiatives we are implementing today will become the baseline for tomorrow. Our constant goal is to continue searching for new ways to manage our processes, find safe and cost-effective solutions and improve clinical outcomes for our patients.
We also found that engaging clinical and technical subject experts and encouraging open forum discussions yielded one more benefit — our employee survey shows a higher level of satisfaction than in previous years. Broward Health organizational culture engages every staff member in search of innovative methods and process improvements. When everyone’s opinion matters, our team can see the positive outcomes of their collective efforts. Together we achieve more.
Boris Kalitenko, MS MIS, CIIP, MCSE, originally from the Soviet Union, completed his training as an emergency room physician in Donetsk State Medical School. He conducted clinical research and published articles in Cardiology Journal and Therapeutic Archive in the late 1980s. Currently he is a senior PACS administrator at Broward Health. Additionally he contributes to system development and integration with other hospitals. He was contributing author to the HIMSS publication “Guide to the Wireless Medical Practice.”
Tom Waters, RTR, has been a technologist for 39 years for two hospital systems in Fort Lauderdale, Fla. Currently he is the regional manager of radiology and interim manager of cardiology at Broward Health Medical Center. He is an active member with the American Society of Radiologic Technologists (ASRT) and American Healthcare Radiology Administrators (AHRA). He serves on the advisory board of two radiology technologist programs.
References:
1 Health Imaging, October 2011, p 14

 April 16, 2024
April 16, 2024 







